


By William Melwyn | WFY Health & Wellness Feature | October 2025 Edition
Silent Struggles: Mental Health, Identity & Belonging in the Indian Diaspora
Beyond the Money and the Mission
For decades, conversation about the Indian diaspora has centred on remittances, economic growth, political influence, and soft power. Fewer people discuss what it means to live between worlds, to succeed outwardly but wrestle inwardly with belonging, identity, and loneliness. Yet across the globe, Indians living abroad increasingly contend with mental health stresses: cultural dislocation, family expectations, silence around emotional well-being, and the weight of representing “home”.
This article draws upon data, studies, and personal narratives to explore how mental health plays out in diaspora communities, the challenges, the stigma, the social forces, and what responses are emerging. The Indian diaspora is not just about money, politics, or fame. It is about human lives navigating multiple identities, histories, and emotional landscapes.
The Hidden Burden: Why Mental Health Matters in Diaspora Life

Migration is rarely a clean rupture. It carries emotional debts: the loss of familiar places, estrangement from roots, unspoken expectations from family, and the pressure to “do well.” Over time, these accumulate into what we might call the emotional shadow of migration.
Research on South Asian immigrants indicates higher rates of psychological distress compared to majority populations, in depression, anxiety, insomnia, and psychosomatic symptoms. (PMC) In the UK, Indian and Pakistani women of older age have shown significantly higher adjusted risk ratios for depression and anxiety than White British women. (PMC) Indian American mental health is under-researched, but latent stigma, underdiagnosis, and cultural idioms of distress mean that many suffer quietly. (Indiaspora)
Indian diaspora voices speak in patterns:
- “I feel guilty that I studied abroad while siblings struggled back home.”
- “I don’t belong fully in either place, I can’t code myself in a slot.”
- “If I admit I’m depressed, family calls me weak.”
The silence is not absence, it is a boundary, a defence, a risk.
Pressures Unique to the Diaspora
Cultural Dissonance and Identity Conflict
Diaspora life often demands code-switching, between languages, social references, values. Some second-generation Indians in Canada or Australia describe feeling “too Indian for locals, too foreign for India.” This bicultural mismatch can spur identity confusion.
Generational gaps widen the tension. Parents may cling to cultural norms (marriage, caste, religion), while children adopt more fluid identities. When mental health crosses paths with these choices, conflict erupts.
“High-achiever” Expectations
Many diaspora Indians are racialised as “model minorities.” There is immense pressure to excel academically, professionally, financially. To admit emotional struggle is to risk being judged as weak or failing. The cultural script often remains: “You came here to do something. Be strong.”
This alone suppresses help-seeking behaviour. Many prefer “hustle through” rather than therapy, or perform silence as resilience.
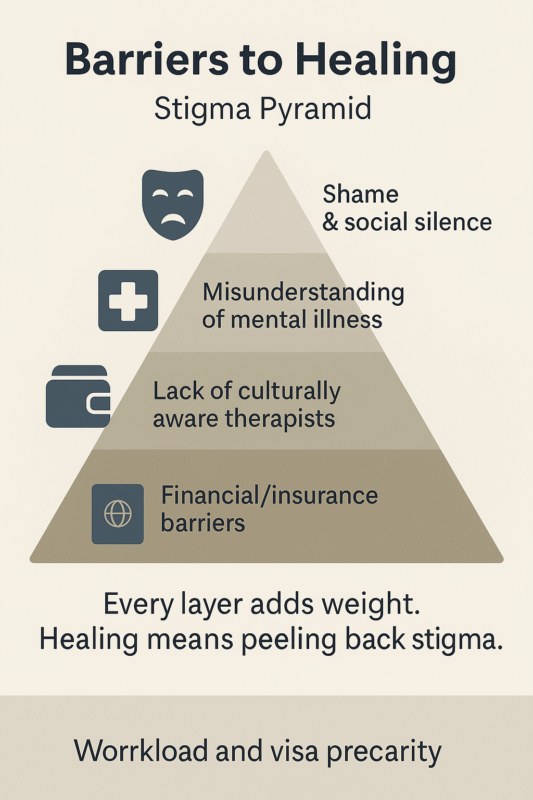
Stigma, Language, and Diagnosis Gaps
Mental health stigma in Indian culture is pervasive: disorders may be framed as “God’s will,” “weakness,” or family dishonour. (PMC) Symptoms may be expressed through physical complaints (headaches, fatigue) rather than psychological language, which mismatches Western diagnostic frameworks.
Therapists unfamiliar with South Asian idioms may misinterpret, misdiagnose, or pathologise. Indian diaspora communities often lack culturally sensitive counselling options.
Acculturation Stress & Discrimination
Diaspora members often face microaggressions, racial bias, and exclusion in workplaces and public life. The daily negotiation of belonging exerts stress. Someone who looks Indian but is acculturated may still be othered.
Immigration anxiety, visa uncertainty, or family separation add additional chronic stressors.
The Data: Prevalence, Gaps & Signals
While comprehensive data on the mental health of Indian diaspora is scarce, existing studies flag alarming trends.
- Psychological Distress Among Asian Indians (Siddiqui et al.) found that among Asian Indian populations in the U.S., mental health issues are often under-disclosed; religious or spiritual frameworks sometimes replace medical diagnosis. (PMC)
- PMC Study on Mental Health in South Asians (incl. immigrants) highlighted elevated rates of depression, insomnia, and anxiety among South Asian immigrants, particularly women, compared to general populations. (PMC)
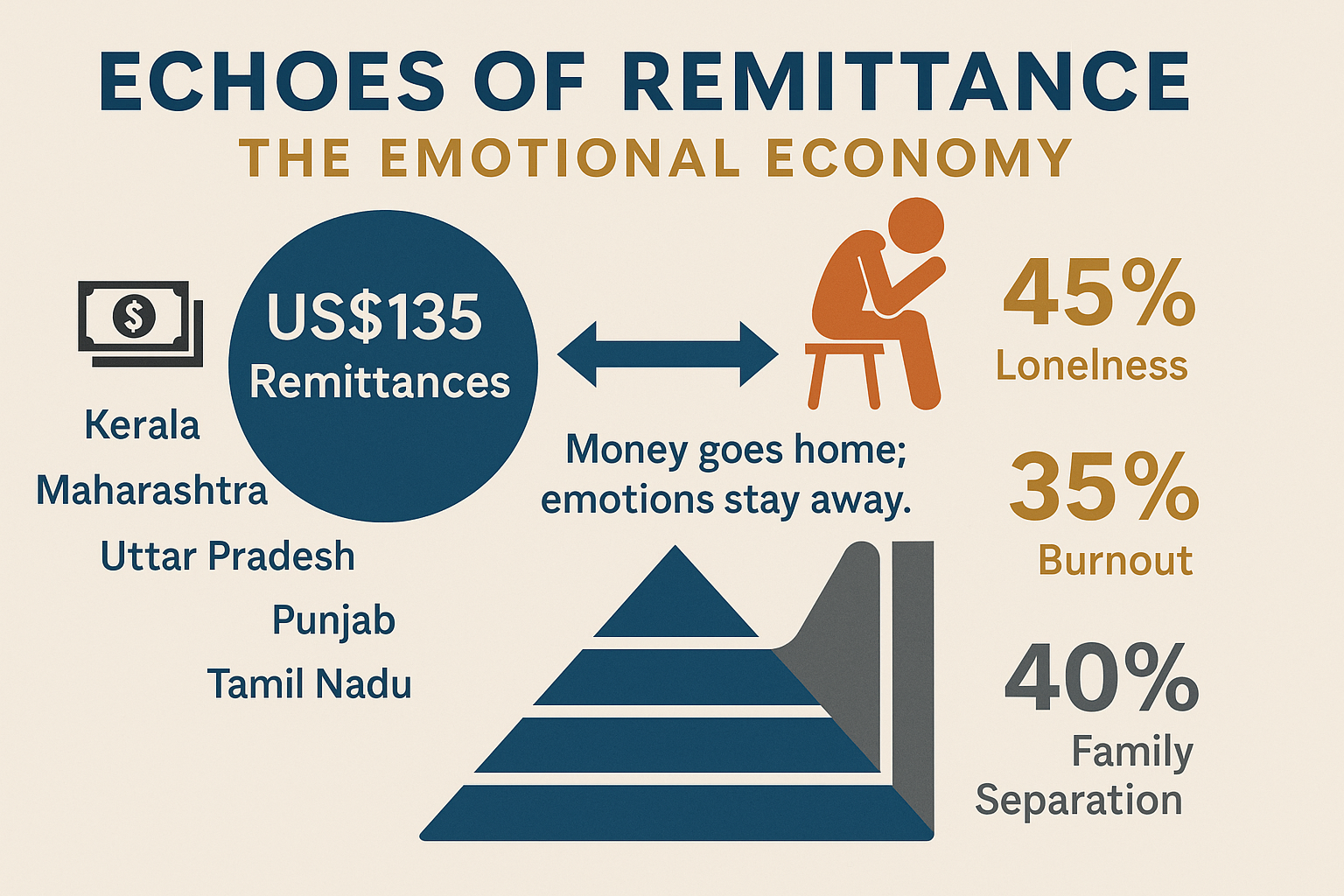
- Indian diaspora remittances, while economic, are also social capital. Remittance inflows to India hit US $135.46 billion in FY24–25, making it the largest recipient in the world. (The Economic Times) Though economic in nature, this flow reflects diaspora’s linkage, and the emotional transactions underlying those connections.
These gaps in data underscore urgency: silence does not mean absence of distress.
The Interplay of Remittances, Family, and Emotional Ties
Remittances are often discussed in economic terms, but they are emotional lifelines. Diaspora migrants carry the weight of families left behind, school fees, medical bills, housing. The expectations are real, heavy, unrelenting.
In rural Maharashtra, a study of remittance-recipient households found that money often supports education, health, and basic consumption. (PMC) But remittances do not mitigate emotional divides. Children growing up without parental presence, extended separation, and silence about anxiety all factor in.
Migration sometimes introduces social remittances, ideas, values, practices flowing back home, not just money. New ideas about gender roles, mental health, civic rights, pluralism, often travel with migrants. (SpringerOpen) But when diaspora individuals struggle, they may withhold or self-censor those social remittances to maintain family harmony.
Stories from the Diaspora (Illustrative Narratives)
Here are composite yet representative sketches drawn from conversations with diaspora friends, community groups, and support networks (names changed):
- Priya, a second-generation Indian in London, studied engineering but battles periodic depression. Her father says “be grateful you’re abroad.” She hides therapy visits from family, fearing shame.
- Anil, a physician in Toronto, lost his sense of purpose when he realised his parents expected him to “give back” to their village. He oscillates between guilt and ambition, rarely admitting burnout.
- Meera, a nurse in Qatar, sends remittances and emotionally distances herself. Her siblings in India tell her she has “become arrogant.” Her longing for acceptance makes her silently lonely.
These lived tensions animate the broader patterns.
Emerging Responses & Community Solutions
Despite silence and stigma, several diaspora and India-based initiatives offer glimmers of hope.
Culturally Informed Therapy & Peer Networks
Some counsellors specialise in South Asian mental health, using bilingual conversation, familiarity with cultural values, and adaptation of Western models. Diaspora support groups (online) for Indians abroad, focusing on anxiety, identity, and acculturation, are slowly growing.
Youth & Student Wellness Initiatives
In Kerala, the “Jeevani” mental health programme offers college counselling services across 66 colleges, reaching ~60,000 students. (Wikipedia) It shows how institutional backing can normalize help-seeking.
The Live Love Laugh Foundation in India works to reduce stigma and promote mental wellness nationwide. (Wikipedia) Diaspora youth often partner with such NGOs to raise awareness across borders.
Diaspora NGOs & Philanthropy
Several diaspora philanthropies now include mental health in their remittance or grant portfolios. The idea is that investing in emotional wellness is as necessary as investing in infrastructure.
Technology-Driven Support
Teletherapy, wellness apps, and diaspora-oriented online platforms offer anonymity and accessibility. As stigma declines, younger diaspora are turning to apps and virtual counsellors.

Structural Challenges & Risks
While these responses offer promise, they face severe structural headwinds:
- Regulation and licensure: Therapy across jurisdictions becomes complicated due to licensing, legal liabilities, and data privacy laws.
- Cultural mismatch: Therapies built for Western populations may not translate well for diaspora Indian idioms of distress.
- Resource scarcity: Many countries have shortages of culturally competent psychologists or limited insurance coverage for mental health.
- Silence and family pressure: Even when services exist, community judgment often stops uptake.
- Disparities within diaspora: Wealthier professionals may access therapy; migrant labourers or lower-income diaspora may lack options.
A Call to Compassion, Connection & Change
The Indian diaspora’s story is not just about human capital and remittances. It is about human capitals, emotional, relational, and psychological. As diaspora grow in scale, we must ask: Are we investing as much in their emotional welfare as we do in their economic roles?
Some guiding principles:
- Normalize conversation: Mental health must become part of diaspora identity talk, not taboo.
- Resist shame culture: Emphasise that emotional struggle is universal, not weakness.
- Support cross-border counselling: Enable therapists to legally offer services across borders, diaspora-friendly telehealth frameworks.
- Culturally sensitive training: Educate mental health professionals about Indian idioms of distress, family systems, faith, and community.
- Youth leadership: Diaspora youth should lead peer networks, storytelling, arts and wellness initiatives.
- Diaspora philanthropy toward well-being: Encourage remittances and grants toward mental health, not just infrastructure.
- Research & data: Governments and academia must fund studies on diaspora mental health, disaggregated by gender, generation, and host country.
From Silence to Solace
The Indian diaspora is often seen through the lens of capital, human capital, financial capital, political capital. Rarely through emotional capital. But the silent struggles, the invisible fissures, are real. They shape identity, belonging, resilience.
Diaspora life demands we listen, to the unspoken, to the pause, to the crack in the narrative where struggle resides. If we want the diaspora to flourish, not only in wealth or influence but in dignity and well-being, then we must turn from silence to solace, from stigma to support.
Mental health is not an afterthought. It is central to the diaspora’s story, its risk, its hope, its humanity.
Diaspora Mental Health: Country Fact Check
United States
- Under-diagnosis among South Asians: Asian patients in U.S. primary care were far less likely to receive anxiety or depression diagnoses than White patients; Asian patients were 227% less likely for anxiety and 213% less for depression, signalling significant under-recognition and access barriers. (Verywell Health)
- Psychological distress signal: A U.S. study on Asian Indians found measurable moderate–serious psychological distress, with authors noting cultural stigma and help-seeking barriers that suppress formal diagnoses. (PMC)
- Community snapshot: US South Asian public-health networks summarise that roughly 1 in 5 South Asians report a mood or anxiety disorder at some point, with low service uptake. Use as an orientation figure, not a national prevalence. (Sapha)
Editorial take: Expect real need + low detection. Many problems sit “below the waterline” because of stigma, language, and provider cultural competence gaps.
United Kingdom
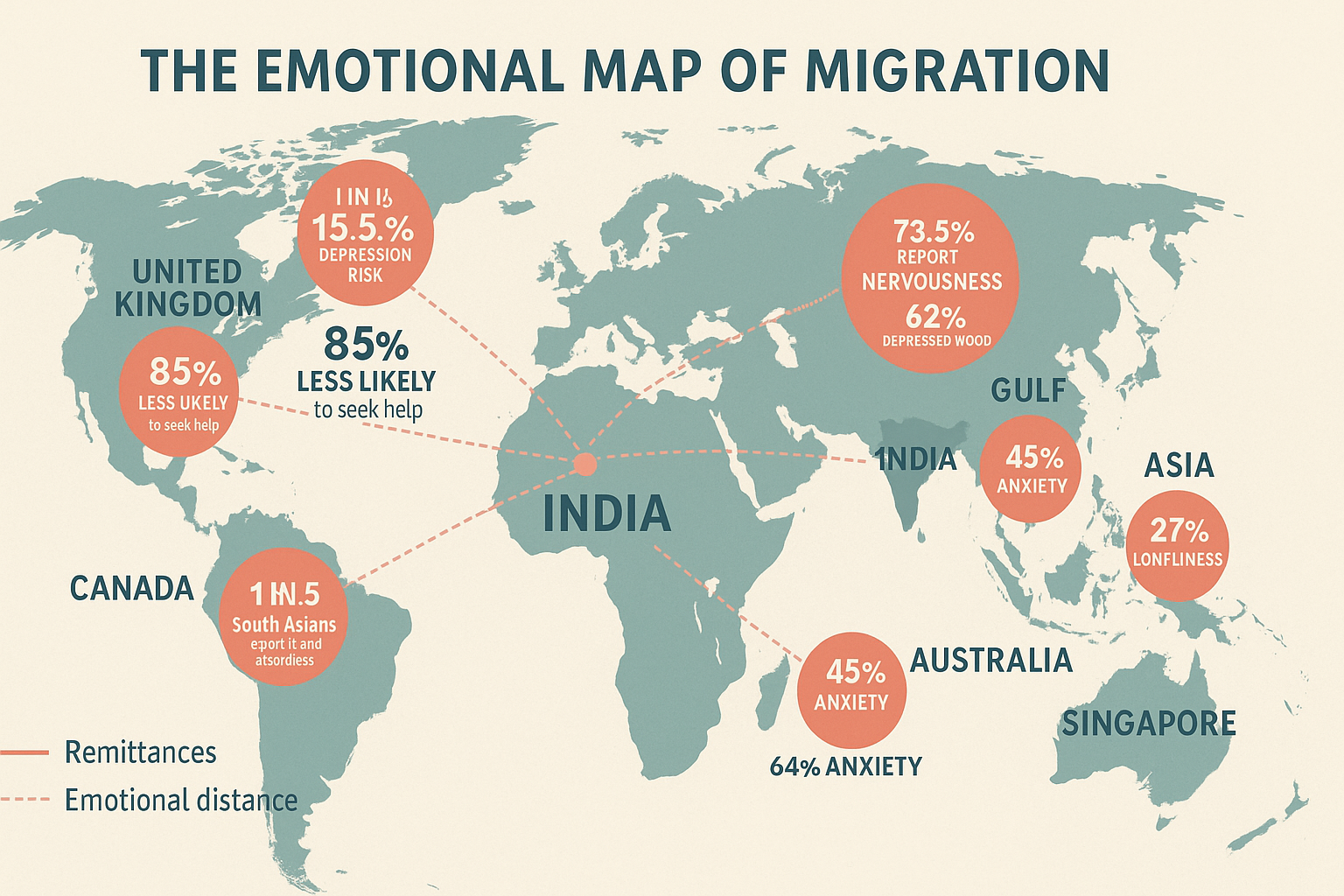
- Older adults: Depressive symptoms were higher in older British South Asians compared with White Europeans in a large study (about 15.5% vs 9.7% respectively). (PMC)
- Across ethnic groups: UK research comparing 18 ethnic groups during the pandemic period shows meaningful differences in common mental disorders by ethnicity, reinforcing the need for targeted, culturally adapted provision for South Asian groups. (ScienceDirect)
- Help-seeking patterns: Qualitative primary-care work finds South Asians often frame distress somatically, which reduces recognition in routine GP settings and delays mental-health referral. (bjgp.org)
Editorial take: High stigma + somatic presentation means conditions are missed unless GPs use culturally informed screening.
Canada
- Higher risk with lower uptake: South Asian Canadians experience higher rates of mood and anxiety disorders than other groups and are about 85% less likely to seek treatment than Canadians with similar illnesses, according to CAMH’s culturally adapted CBT programme brief. (CAMH)
- National lens: Statistics Canada’s MHACS 2022 release tracks who meets diagnostic criteria and who actually accesses care; it documents persistent unmet need in mental-health services nationally, a context in which South Asian disparities sit. (Statistics Canada)
- South Asian immigrant evidence base: Reviews focused on South Asians in Canada report elevated anxiety and depression risks relative to majority populations and consistent service under-utilisation tied to cultural and structural barriers. (PMC)
Editorial take: Canada shows a clear access gap. Community outreach and culturally adapted therapies move the needle.
Gulf (UAE, Saudi Arabia, Qatar, Oman, Kuwait)
- Indian migrant workers in UAE (post-pandemic snapshot): 73.5% reported nervousness, 62% depressed mood, 77% loneliness, 63.4% sleep problems, and 63% concentration problems in a 2023 survey of Indian migrants. (PMC)
- Meta-estimates for migrant workers in GCC: Pooled prevalence suggests ~21% depression among migrant workers, with wide variance by setting and method. (Medical and Research)
- Global migrant-worker evidence: Systematic reviews describe increased incidence of anxiety, PTSD, and serious mental disorders linked to debt bondage, overcrowded housing, heat stress, and family separation. (MDPI)
- Evidence gaps: Earlier Gulf reviews noted high psychosis and suicide reports but limited reliable surveillance, underscoring the need for better data collection. (ScienceDirect)
Editorial take: The Gulf story is about precarity. Risk factors are structural: recruitment debt, long hours, isolation, and visa dependency.