By WFY Bureau | Health & Wellness Feature | October 2025 Edition
The Longevity Paradox: Why Indians Abroad Are Living Longer, Yet Feeling Unhealthier
Introduction: The Paradox of Modern Health
In 2025, Indian-origin communities across the world stand at an intriguing crossroads. They are living longer than their counterparts back home, enjoying higher incomes, and benefiting from advanced healthcare systems. Yet, paradoxically, they report higher rates of chronic stress, cardiovascular disease, diabetes, and mental health struggles. The so-called “model migrant” success story hides a more complex truth: longevity without wellness.
Indian diaspora populations, spread across more than 200 countries, number nearly 35 million, and the largest expatriate community on the planet. They are, by many indicators, thriving. But a closer look reveals a troubling pattern. Doctors in London, Toronto, Dubai, and New York are treating a rising number of Indian-origin patients for hypertension, obesity, depression, and Type 2 diabetes, often in their 30s and 40s.
This feature examines why a generation that seems outwardly prosperous is silently paying a heavy health price, and how lifestyle, identity, stress, and systemic neglect together shape the new epidemic of diaspora ill-health.
The Numbers Tell a Story
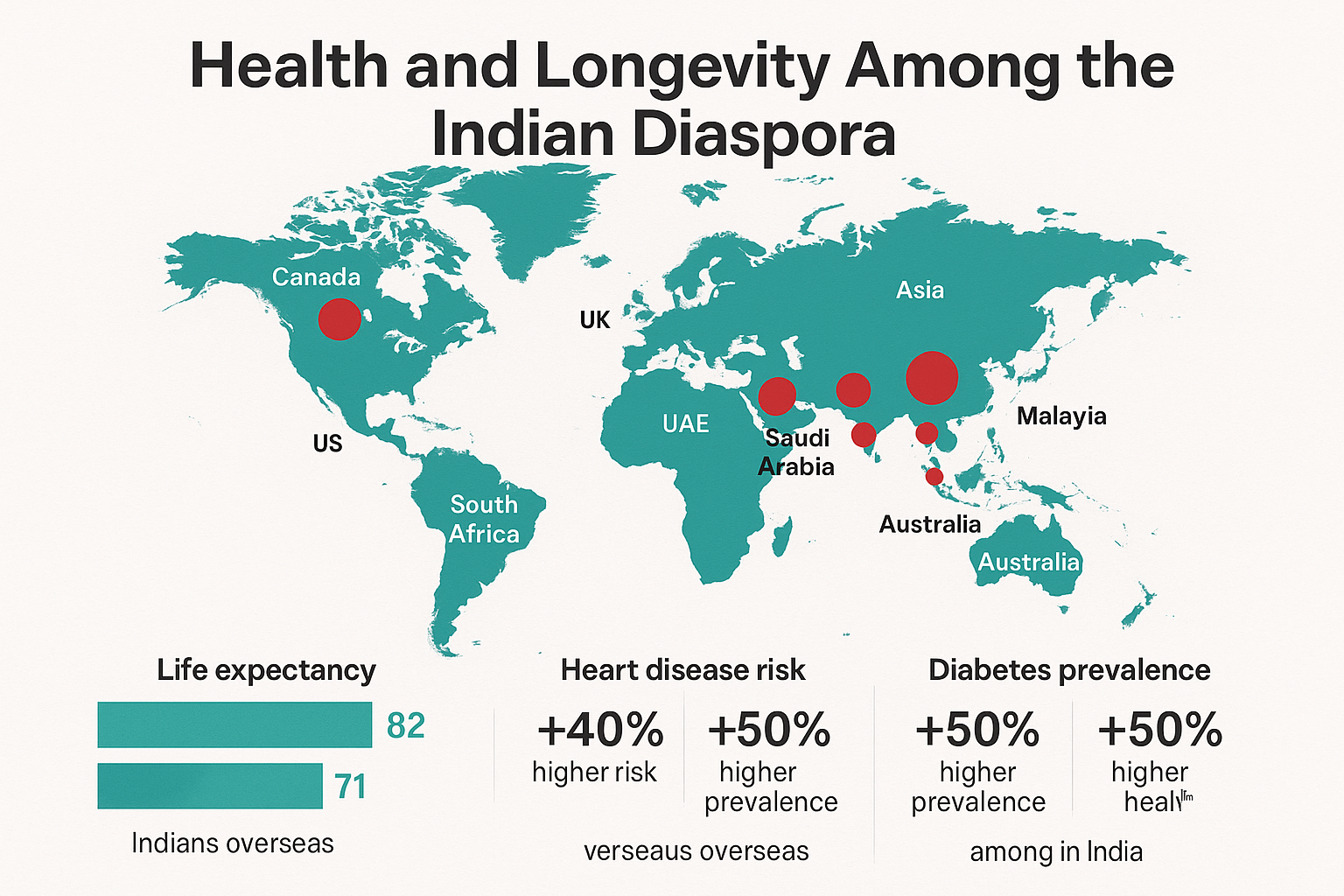
- Life expectancy: Indians abroad, on average, live 6–9 years longer than residents of India, according to WHO global migration health studies.
- Chronic disease: However, South Asians have a 40–60% higher risk of heart disease compared with Western populations at the same BMI level.
- Diabetes prevalence: Among Indian-origin adults in the UK and US, the rate of Type 2 diabetes is nearly double that of native populations.
- Obesity: In Canada and Australia, obesity rates among Indian immigrants have tripled since 2000.
- Mental health: Studies show that 1 in 5 Indian diaspora adults experiences anxiety or depression, yet less than a quarter seek professional help.
These figures paint a stark contrast. Better access to healthcare doesn’t necessarily mean better health. And that contradiction lies at the heart of the diaspora’s wellness crisis.
The Biology of Migration
When Indian migrants move to wealthier nations, they gain access to better diets, healthcare, and living standards. But biologically, their bodies are primed for thrift. Centuries of food scarcity and adaptation have shaped a “South Asian phenotype”, a body built to store fat efficiently.
This genetic inheritance, beneficial in pre-industrial India, becomes a liability in the high-calorie, sedentary lifestyles of the West. Nutritionists refer to it as the “thin-fat syndrome”, Indians appear slim externally but carry dangerous visceral fat around vital organs, increasing their risk of metabolic diseases.
Recent research by the Harvard T.H. Chan School of Public Health shows that South Asians develop insulin resistance and heart disease a decade earlier than Caucasian peers, even with similar diets. Add to this long working hours, irregular meals, and chronic stress, and the body begins to rebel.
The Western Lifestyle Trap
Migration often means upward mobility, but it also brings drastic lifestyle shifts. Traditional Indian diets rich in pulses, grains, and vegetables are replaced with processed convenience foods and sugary drinks. The typical weekday of an Indian professional abroad might look like this:
- Skipped breakfast.
- Coffee-laden mid-morning.
- A quick sandwich lunch at the desk.
- Late-night dinners after long commutes.
In North America and Europe, this pattern, combined with reduced physical activity, has turned middle-aged diaspora professionals into high-risk groups for metabolic syndrome.
A 2024 study across 12,000 South Asian expatriates in the UK found that 63% had abnormal cholesterol, 47% were pre-diabetic, and 31% were hypertensive. Many had normal body weight but high waist-to-hip ratios, the classic indicator of “hidden obesity.”
Work-life imbalance
Diaspora Indians, especially in competitive sectors like technology, finance, and medicine, often work longer hours than their native peers. According to LinkedIn’s 2024 Global Workforce Index, Indian-origin professionals in the US logged an average of 51 working hours per week, compared to the American average of 44.
The cultural ethos of “keep working, keep providing” leaves little space for rest or recreation. While such discipline contributes to career success, it erodes physical and emotional reserves, a silent burnout masquerading as ambition.
Stress, Identity, and the Hidden Mental Toll
Behind the polished success stories lies an emotional reality: displacement, cultural duality, and isolation.
First-generation migrants often feel torn between two worlds. Second-generation youth face identity confusion, neither fully Western nor fully Indian. For both, the struggle for belonging manifests as psychological distress.
A 2023 British Journal of Psychiatry review found that Indian-origin adults in the UK were 1.6 times more likely to experience depression than white British adults, yet far less likely to access mental health services. In the US, South Asian suicide rates among young adults rose by 32% between 2010 and 2020, the steepest increase among any ethnic group.
In the Gulf, the story is harsher. Among Indian migrant labourers, suicide remains one of the top causes of death. Living in overcrowded accommodations, facing job insecurity, and being separated from families for years, these men internalise despair until it manifests in tragedy.
“Diaspora depression” is no longer a poetic metaphor. It is a public health issue.
The Diet Dilemma – Tradition Meets Convenience
Ironically, while global interest in Indian cuisine has exploded, Indians abroad are eating less of the food that once kept them healthy.
Traditional thalis with lentils, rice, vegetables, and curd offered fibre, plant protein, and probiotics. The Western diet, high in sugar, salt, and saturated fat, replaces them with instant noodles, frozen parathas, and takeaways.
Dietitians in the UK report a surge in gastrointestinal disorders among Indian immigrants, especially vegetarians who shift to high-carb processed meals. Vitamin D deficiency, anaemia, and low calcium levels are now common among younger professionals.
Moreover, the habit of overcooking vegetables, inherited from Indian kitchens, reduces nutrient retention. Add late-night dining and reduced physical activity, and the metabolism suffers a continuous assault.
The Silent Killer – Heart Disease and Diabetes
Cardiovascular disease is now the leading cause of death among Indian-origin people worldwide. A study by the British Heart Foundation found that South Asians are 50% more likely to die of heart disease than other ethnic groups.
In the U.S., despite higher education and income levels, Indian Americans have a twofold higher risk of coronary artery disease. The problem is not only biological but behavioural: late meals, chronic stress, and minimal exercise.
The Gulf nations present a different but equally worrying picture. Among Indian expatriate workers in the UAE, nearly 25% are diabetic, many undiagnosed until hospitalisation. The combination of poor diet, extreme work hours, and limited healthcare access creates a silent epidemic.
Women’s Health – The Invisible Frontier
Indian women abroad often shoulder dual burdens, professional pressure and cultural expectations of caregiving. Yet, they remain an under-discussed demographic in diaspora health studies.
A 2024 Canadian survey found that South Asian women were twice as likely to report chronic fatigue and depressive symptoms compared with men of the same background. In the UK, rates of gestational diabetes among Indian-origin women are three times higher than the national average.
Social conditioning discourages open discussion about menstruation, menopause, or sexual health. Many women skip preventive screenings like mammograms or pap smears due to embarrassment or misinformation.
Community outreach programs, when culturally adapted, show promising results. For instance, the “Sehat” initiative in Birmingham, led by South Asian women doctors, increased breast cancer screening compliance among Indian-origin women by 42% in two years.
The New Generation – Fitness or Fixation?
Second-generation Indians in the diaspora show a curious divide. Some embrace wellness trends, yoga, plant-based diets, and mindfulness, reclaiming ancestral practices. Others drift toward extremes: body-image obsession, crash diets, and substance use.
In the U.S. and Canada, Indian-origin teenagers have among the highest rates of vitamin D deficiency due to reduced sunlight exposure and indoor lifestyles. Social media-driven comparison culture amplifies anxiety.
The irony is that while wellness has become fashionable, genuine health, balance, sleep, and community, remains elusive.
The Gulf Reality – Health Without Rights
For Indian migrant workers in the Middle East, health is not about lifestyle choice but survival. Most live in crowded dormitories, with poor ventilation and limited access to medical care. Long working hours in extreme heat, coupled with poor diets, result in dehydration, hypertension, and musculoskeletal disorders.
A 2023 International Labour Organisation study found that 67% of Indian construction workers in Qatar had untreated chronic conditions, and 18% had symptoms of depression. Yet only a fraction ever saw a doctor.
The problem is systemic: visa restrictions, language barriers, and fear of job loss discourage workers from seeking medical help. For this segment of the diaspora, wellness begins with rights, the right to rest, healthcare, and dignity.
The Myth of “Western Medicine Will Fix It”
One common misconception among diaspora families is that advanced healthcare abroad guarantees better outcomes. In reality, prevention remains the missing link.
Doctors report that many Indian-origin patients seek medical attention only after major complications arise. There is also a tendency to self-medicate, rely on home remedies, or dismiss early warning signs as “just gas” or “tension.”
Moreover, South Asians metabolise certain drugs differently, for example, statins and beta-blockers may require dose adjustments. Yet few patients inform doctors about their Ayurvedic or herbal supplement use, creating risky drug interactions.
Towards a Culture of Preventive Health
What can change this trajectory? Experts suggest three fronts: awareness, accessibility, and adaptation.
1. Awareness
Education about preventive screenings, balanced diets, and early intervention is vital. Community media, including diaspora magazines like WFY, can play a transformative role.
2. Accessibility
Health systems in the West must invest in culturally competent care: hiring multilingual staff, training clinicians about South Asian health risks, and building trust through community partnerships.
3. Adaptation
Indian-origin communities need to rediscover sustainable traditions, walking after meals, eating fresh, observing seasonal rhythms, rather than chasing Western wellness fads.
The rediscovery of yogic science, Ayurvedic dietetics, and community-based mindfulness has real potential when stripped of commercial gimmicks and applied with discipline.
The Diaspora Doctor Movement
A heartening trend is the rise of Indian-origin doctors leading public health reforms in their adopted countries.
In Canada, South Asian physicians launched the “Brown Health Project” to research genetic risk profiles unique to Indian populations. In the UK, the “Desi Heart Study” has produced new screening tools for early heart disease detection.
Meanwhile, Indian cardiologists in Dubai and Singapore are setting up preventive clinics focusing on lifestyle coaching rather than medication alone. The diaspora, once seen as patients, is slowly becoming the healer.
The Wellness Renaissance – Back to Roots, Ahead with Science
Across diaspora hubs, wellness movements are taking hybrid forms. Yoga studios in New York now blend ancient asanas with neuroscientific mindfulness. Indian vegetarian restaurants in London promote “gut balance menus.”
The second-generation youth are redefining what health means, not just survival or physical endurance, but harmony of mind and identity.
However, wellness cannot be outsourced to apps or weekend retreats. It begins with everyday discipline, eating mindfully, resting adequately, nurturing community bonds, and de-stigmatising vulnerability.
Lessons for India, Lessons from Abroad
Ironically, the diaspora’s health struggle mirrors India’s own urban reality, sedentary lifestyles, stress, and rising non-communicable diseases. The difference is that the diaspora faces an additional burden: cultural isolation.
India can learn from diaspora data to build targeted preventive strategies, while diaspora communities can borrow India’s emerging low-cost health innovations, telemedicine, wellness tech, and community health workers.
Towards Wholeness
The Indian diaspora’s journey is a triumph of resilience. But in chasing success, many have neglected the quiet work of self-care.
Longevity without quality of life is a hollow victory. Wellness, for a people who crossed oceans to build better futures, must mean more than survival. It must mean harmony, with body, mind, and community.
In the coming decade, as diaspora Indians become more visible in global leadership, their greatest strength will not be economic power or intellect, but the courage to redefine health as balance, not burnout.
The future belongs not to those who live longest, but to those who live fully.